
Risk Factors
There are numerous risk factors that contribute developing coronary heart disease. Many contribute to atherosclerosis.
Some you can control and some you can't, and it's normally the prevention of as many of these risk factors as possible
that can reduce the indicence of developing CHD.
It's also important to realise that although some factors are considered controllable, there are some people who will be
unfortunately still prone to the risks. There may be more but the main factors are as follows:
- Age
- Sex (Females are more resisant!)
- Socio-economic group/occupation
- Inherited predisposition
- Diabetes Mellitus
- Hypercholesterolaemia (High cholesterol)
- Hypertension (High blood pressure)
- Obesity/weight
- Tobacco use
- Diet
- Lack of physical excercise
- Stress/Depression
- Chlamydia (though not definite)
Brief explanation of how each of these factors contribute are below, though many overlap.
Age
Research has shown that fatty streaks in the coronary arteries begin to develop in childhood. Often, the childhood habits
effect the development of these streaks many years later in life. As age increases, the risk of suffering the effects of
CHD become more visible. Epidemiological studies have also shown that mortality from CHD is higher with increased age.
Increased age as a risk factor could also be due to greater life expectancy and improving health treatments, delaying
the incidence of CHD to later in life.
Sex
Epidemiologic studies have also shown that men have a higher mortality and morbidity rate than women. Pre-menopausal
women tend to have higher levels of HDL compared to men of the same age. This could be due to oestrogen has an effect on
lipid metabolism, causing LDL levels to reduce and HDL levels to rise. Higher levels of HDL is considered protective
against atherogenesis.
Socio-economic group/Occupation
Lower socio-economic group,poverty and low income has been found to be associated with a higher risk of incidence and
mortality from CHD. Although, this is not an absolute factor. But this factor umbrellas education, access to healthcare,
housing and stress. Low qualities of these would tend to result in poor health.
Inherited predisposition
This put simply means, genetics! History in the family of atherosclerosis is often inherited. Moreoever, history of
other risk factors such as hypercholesterolaemia or diabetes can increase the risk of cardiovascular diseases in an
individual. Therefore, family history is a very important tool in the screening and diagnosis of CHD.
This risk factor also includes ethnic background. South Asians in particular are at higher risks of developing
cardiovascular diseases.
Diabetes Mellitus
Typically Type II (non-insulin dependant) is the major factor. Diabetes effects many metabolic pathways in the body and
itself can lead to other conditions, which are also considered risk factors. Diabetics often have dyslipidaemia and
hyperglycaemia, hypertension and hypertriglyceridaemia. High levels of triglycerides can lead to smaller and more dense
LDL as well as reducing levels of HDL, hence, increasing risk of CHD. Hyperglycaemia, in diabetes, has been found to
induce formation of advanced glycation-end products (AGEs) which can in turn induce inflammatory responses in
atherosclerotic lesions.
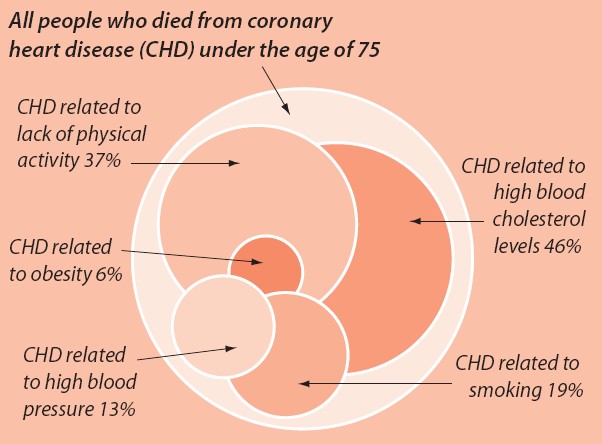
Hypercholesterolaemia
High plasma levels of cholesterol, by high levels of LDL for example, increase the chance of excess deposition of
cholesterol onto the endothelial walls of the coronary arteries. One of the first steps in atherogenesis!
Recommended levels:
|
Total Cholesterol: Triglycerides: HDL Cholesterol: LDL Cholesterol: |
< 5.0 mmol/l 0.4-1.8 mmol/l 0.7-2.1 mmol/l < 3.0 mmol/l |
Hypertension
High blood pressure causes the heart to work harder. It may initiate atherosclerosis by causing damage to epithelial
cells of the coronary arteries. However, hypertension in combination with other risks factors only speeds up
atherosclerosis.
Blood pressure around 120/80 mmHg is considered Normal.
Blood pressure above 180/100 mmHg is considered High!
Obesity/Weight
 Measurement of obesity is often quantified by calculation of an idividual's BMI. Obesity itself can cause a multitude of conditions! For example, it can raise blood cholesterol
levels and blood pressure, causing the heart to work harder.
Measurement of obesity is often quantified by calculation of an idividual's BMI. Obesity itself can cause a multitude of conditions! For example, it can raise blood cholesterol
levels and blood pressure, causing the heart to work harder.
BMI > 30 kg/m2 is classified as clinically obese, and must lose weight.
BMI 25-30 kg/m2 is classified as overweight.
BMI 20-35 kg/m2 is the Desirable Range.
BMI < 20 kg/m2 is underweight.
Tobacco use

Smoking on itself also causes a range of conditions, some fatal. Byproducts of tobacco (e.g. nicotine and CO) may cause
damage to epithelial cells in the coronary arteries. Also, tobacco smokers have higher levels of fibrinogen, a protein
involved in clotting, so causing the arteries to harden. Smokers have also been found to have lower HDL:LDL ratios. Also,
the public ought to be aware of its effects on cancer and fatal myocardial infarctions. Hence, smoking is a high risk of
CHD, as well as other cardiovascular conditions. Second-hand smoke can still cause cardiovascular problems, though may
not be as severe.
Diet
The food we eat is the major source of what goes into our body. Fast foods, or food with high saturated fat or high
trans-fatty acid content promote atherosclerosis by increasing the lipid content in our body. Not to mention, also
causing obesity. Excess alcohol consumption, as well as having toxic effects on the heart, leads to conditions that go
on to promote the development of CHD.
Lack of physical excercise
Lack of excercise is a factor that becomes more common with increasing age, but, excercising has huge benefits! Lack of
excercise can lead to obesity, poor metabolism, high cholesterol and hypertension. The anti-atherogenic effects of
physical excercise is explained on the Prevention page.
Stress/Depression
Stress and depression, as a fact, is known to effect the body's metabolism and immune system by release of
chemicals/hormones such as adrenaline and cortisol. Adrenaline can cause blood vessels to constrict and raise blood
pressure. This bad news for someone who already has a plaque-filled lumen from atherosclerosis! Vasoconstriction worsens
the effect and can lead to ischaemia - noticed as the pains of angina. Stress may also cause retension of cholesterol
in the body, a factor increasing chance of atherosclerosis.
References [Show/Hide]

Royal Free & UCL Medical School